Research Highlights
Mechanisms of Adolescent Suicidal Thoughts and Behaviors

Suicide is a major public health crisis and is the second leading cause of death among 10-24-year-olds. Suicidal thoughts and behaviors increase drastically during adolescence and are particularly common in adolescent depression. However, it is unclear why certain depressed adolescents engage in suicidal behaviors. Current models suggest that there are predisposing factors, such as childhood trauma, and acute factors, like social rejection and interpersonal loss, that increase risk. Neither factor alone is likely sufficient, rather predisposing factors and stressors must be considered together to clarify suicide risk. Reviews highlight potential neural risk factors, including striatal reward responsivity, prefrontal regulatory circuits, and modulatory neurotransmitters. Yet, in a recent review of the literature, we found that MRI studies aiming to understand adolescent suicide risk are lacking; we highlight potential steps forward including examining interacting effects of stress and using ambulatory assessment methods. In a research paper, we examined data from a large sample of adolescent in inpatient psychiatric care; suicidal thoughts and behaviors were exceedingly common and typically began in early adolescent. Depressive disorder and abuse histories were related to greater likelihood of suicide attempt as well as knowing a peer who had also attempted suicide.
Neural Markers of Psychiatric Risk in Youth

Many studies have documented the contributions of family history to increasing psychiatric risk, e.g., youth with a parental history of depression are ~2-3x more likely to experience depression (and anxiety) themselves than those without a family history. Yet, more work is needed to understand how family history confers this risk and what factors might protect against familial risk. Particularly, it is critical to examine the neural mechanism of psychiatric risk in children prior to the typical peak onset of disorder to separate sequalae from predisposing risk factors. Examining the large ABCD Study, we have reconfirmed this association between parental depressive history and increased depression & anxiety risk in children as young as 9; furthermore, parental history was related to smaller putamen volumes in children. Work with Dr. Katherine Luking has shown that maternal depression history is also linked to less neural sensitivity to winning money but enhanced response to losing. A maternal depression history also relates to increased risk for prolonged irritability across child development; typically, young children exhibit irritability that wanes over development, but this is more likely to persist among those with a family history. In work at the NIMH, we found that youth and young adults with bipolar disorder or with only a family history exhibit more variable responding on a selective attention task; lapses in attention were mediated by robust alterations in fronto-striatal activation differences.
Moderators and Mediators of Stress Effects on Mental Health
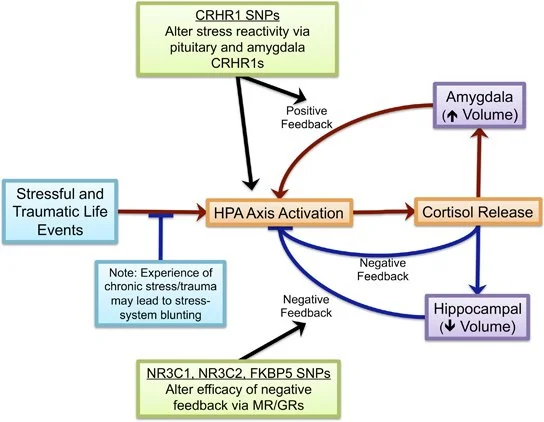
Many studies have documented adverse psychiatric outcomes of stressful experiences, particularly during early childhood. Yet, not all those who experience stress experience mental health concerns later in life. A diverse set of moderating factors can influence the effect of stress on the brain and mental health in youth. Further, the mechanism by which early life stress influence the brain and thereby psychiatric risk are still under investigation. My work has shown that an additive profile of stress-system genetic variants, while each of small effect, had a cumulative risk effect on cortisol function and a moderating role in impacting brain structure, function, and connectivity in children. Further, I have found that exposure to environmental toxicants, even in utero, can sensitize the system to the effects of stress on adverse psychiatric outcomes.
Contribution of Neural Markers to Outcome Prediction

Identifying robust predictors of mental health outcomes both longitudinally across development and following treatment would be critical advances. This would allow for identification of at-risk youth most needing of early intervention or prevention efforts and would facilitate guidance of affected youth to the most efficacious treatments. Neural markers may be a critical means to improve outcome prediction beyond baseline factors, like baseline symptoms. This work has identified a number of potential structural and functional neural markers that may be useful in predicting outcomes. We have found that task-based fMRI relates to cognitive behavioral therapy outcomes in adults with OCD, particularly in cingulo-opercular and default mode network regions. This further was partially mediated by patients adherence to exposure and response prevention treatment. Among youth with OCD, structural MRI, particularly cortical thickness in fronto-parietal regions, as well as amygdala functional connectivity elated to therapy outcomes. In the large ABCD study, we found that obsessive compulsive symptoms related to dorsal attention connectivity, and connectivity between this network and the default mode network related to change in symptoms over the next one year.
Methodological and Psychometric Advances

Throughout my research career, I have aimed to utilize strong and well-validated methods. In studies of brain imaging, particularly with children, much more work is needed to ensure that the best and most reliable measure of brain function are being examined as well as ensuring that the psychological measures that we employ have been fully vetted and validated for use in children. Examining an fMRI study of emotional face processing, one of the keystone paradigms for studying affective processing, I was able to show that the amygdala in school-age children does not differentially respond to expressions different facial emotions. This is in contrast to a majority of adult studies showing differential responding to neutral and fearful expressions and calls for further study of this paradigm and stimuli as well as developmental progression of these processes. In forthcoming work, we examine the test-retest reliability of face emotion paradigms; cross-scanner differences are minimal, but reliability overtime is weak in many regions of interest. Reliability is stronger for contrasts of more distinct conditions, and is strong in visual regions, such as the FFA. Then, in prior and on-going work, I have helped to examine the psychometric properties of two often utilized questionnaire measures. This work has helped to clarify the developmental validity of the BIS/BAS measure and suggested changes to the scoring of this measure for use across children and adults as well as examining parent-child discrepancy of reporting as well as validity of the SCARED measure of anxiety.